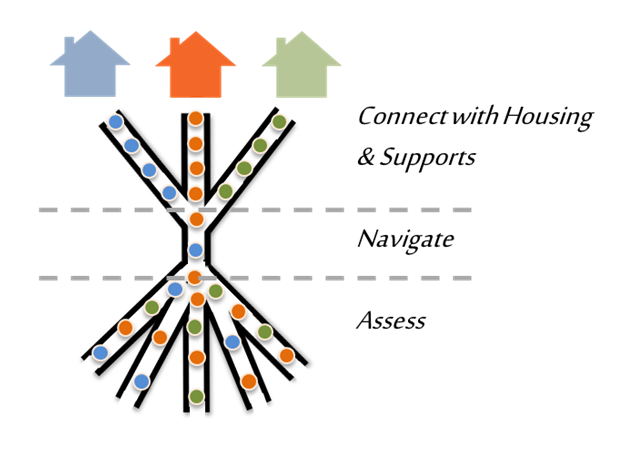
Over the past year the County of Marin, local service providers, and the City of San Rafael have begun adopting a dramatically new strategy for ending chronic homelessness. This new approach is called “Coordinated Entry,” and it has been pioneered, vetted, and proven successful in communities around the country.
This is Part 1 of a three-part series that will breakdown the strategy we’re now pursing to end chronic homelessness in San Rafael and Marin.
Focusing on Chronic Homelessness
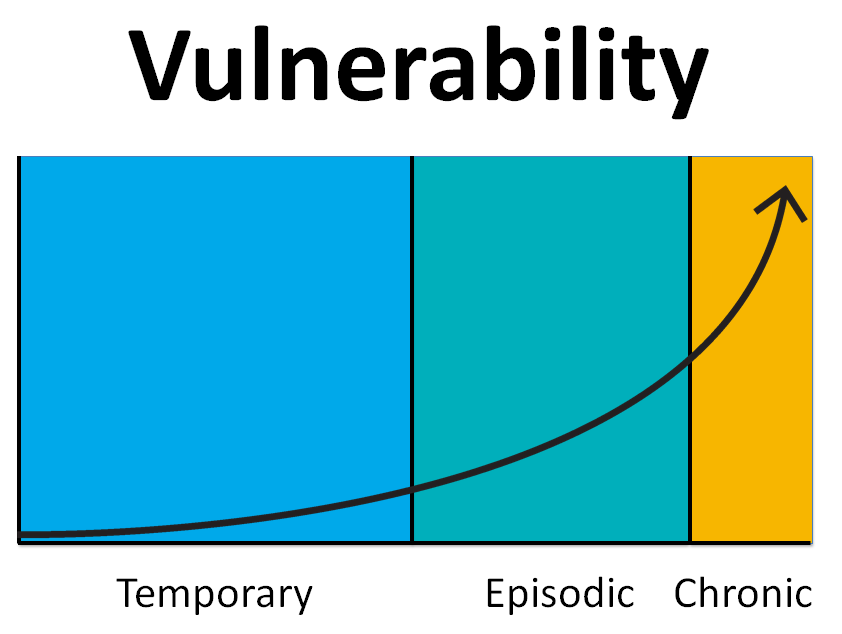
Chronic homelessness is defined as long-term homelessness (> 1 year) accompanied by a debilitating condition (serious mental illness, severe substance abuse, traumatic brain injury, development disabilities – or, typically, multiple issues at once). Though less than 20% of the homeless community is chronically homeless, they typically account for 80%+ of our challenges.
The average chronically homeless person:
- Generates a significantly disproportionate number of 911 calls and community complaints
- Dies 20 years earlier than housed peers due to chronic health conditions
A Critical Insight from Emergency Rooms
Imagine I’m cooking dinner one night, and I cut my hand. It’s far from life-threatening, but I definitely need stitches, so I decide to go to the ER. Just as I’m finishing my paperwork, the doors of the ER fly open and YOU get wheeled in on a stretcher. You’re having a heart attack.
In this scenario, who would be treated first? You, of course.

The healthcare industry triages a person’s individual needs and then prioritizes care based on the level of life-threatening severity. For the last 35 years we have used the exact opposite approach with homelessness. Not always, but often:
- If I’m first in line, I get served first.
- If I’m articulate and good at telling my story, I get served first.
- If I’m annoying and pester you, I get served first.
- If I’m not well-behaved, I don’t get served at all.
In comparison, think about a hospital. If I’m having a heart attack, it doesn’t matter if:
- I’m rude and disrespectful.
- This is my second heart attack, and I didn’t follow your advice from last time.
- People with non-life threatening injuries came in before me.
In all of these cases, my situation is more severe than others’, so I get treated first.
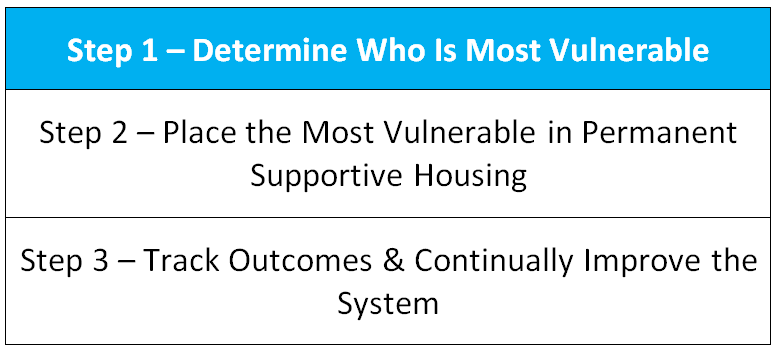
The Process Starts with a Standardized Assessment Tool
To identify the most in need, we need a standardized assessment just like the triage tools nurses and doctors use. Imagine if every doctor or nurse used a different intake method for evaluating patients. It’d be chaos, right?
Unfortunately for the last 35 years, almost every nonprofit and government agency has had their own unique way of entering people into their system. It’s confusing for the person in need, and it’s inefficient for our system of care.
To address this problem, communities across the country are using something called the Vulnerability Index-Service Prioritization and Decision Assistance Tool (VI-SPDAT). Despite being the most ridiculous acronym I’ve ever encountered, the VI-SPDAT is an easy to use questionnaire that generates a score between 0-16. Here’s a sample of some of the questions:
- In the past 6 months, how many times have you been to the emergency room?
- Have you been attacked or beaten up since becoming homeless?
- Do you have any legal stuff going on right now that may result in you being locked up or having to pay fines?
A New Process for Housing Referrals
The fundamental insight for the VI-SPDAT is that certain score ranges point to certain housing interventions. Most people who become homeless are extremely resilient, and they are able to get themselves out of homelessness relatively quickly with minimal support. However, some people need more long-term care and assistance. Without a standardized assessment, “low-needs” people often end up in “high-needs” services, or vice versa. To put this another way, if I only needed stitches, I shouldn’t be hospitalized over night for an MRI scan. The VI-SPDAT is an objective way to help our system of care determine how best to deploy our limited resources and get people the most effective level of care.
If 16 is the most vulnerable and 0 is the least, then:
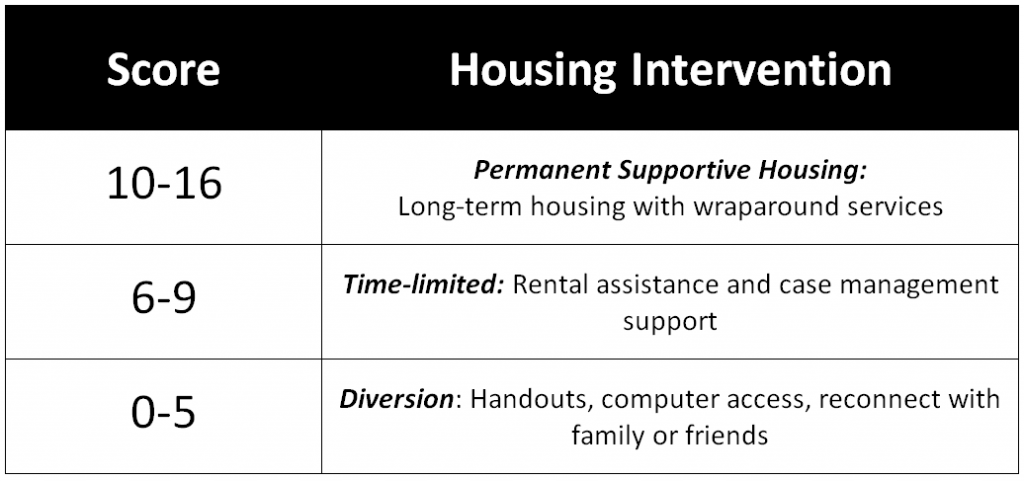
Putting It All Together
The County of Marin and our service providers – Homeward Bound, St. Vincent’s, Marin Housing Authority, and Ritter Center to name a few – have made tremendous progress implementing this new system:
- Spring of 2017 – Approved the use of the VI-SPDAT
- May 10th – Approved the use of a new release of information to share data across organizations
- May 26th – Launched new data software to coordinate across programs
This fall, Marin County will receive $113,493 from the Department of Housing and Urban Development to finalize the implementation of this new assessment system. With that funding and the steps we have already taken, our system of care will be operating at an entirely new level.